
An honest assessment of Medicare for All
There’s no getting around voters’ deep-seated opinions
Every election cycle I’ve worked in polling, I’ve seen different factions of the Democratic Party debate whether voters want a single, federally administered health insurance program. And each time, I’ve asked voters about it. At this point, I’m extremely familiar with the central dynamic around the issue: “Medicare for All” as a term is generally popular, while the actual proposal commands less support.
Last week, Searchlight collaborated with Zeteo, a progressive new media organization, to ask voters whether they’d support the federal government playing a larger role in the American health care system. We asked a variety of questions regarding coverage for pharmaceutical drugs, surgeries, etc., and found that voters overwhelmingly wanted more government intervention. On the question of Medicare for All, however, the results were mixed.
Both of our organizations support expanding the role of the federal government in providing health care coverage. The difference is that Zeteo advocates for Medicare for All, while Searchlight has a plan that achieves many of the same policy goals in a manner that we believe is more pragmatic and mindful of voters’ deep-seated opinions.
I’m a progressive and I want to see the federal government provide more quality care at lower cost. But I’m also a pollster who has spent years grappling with public opinion. Support for Medicare for All varies a lot depending on question wording; the more you spell out the details of the program and what it would require, the more voter support for the policy drops. The questions we developed with Zeteo were developed as a compromise between two organizations with two competing visions of what health care could look like in this country.
What do voters think about single-payer health care?
Since voters’ opinions change depending on exactly how you word the single-payer plan, we split our poll into three equal groups and asked voters questions with three different wordings.
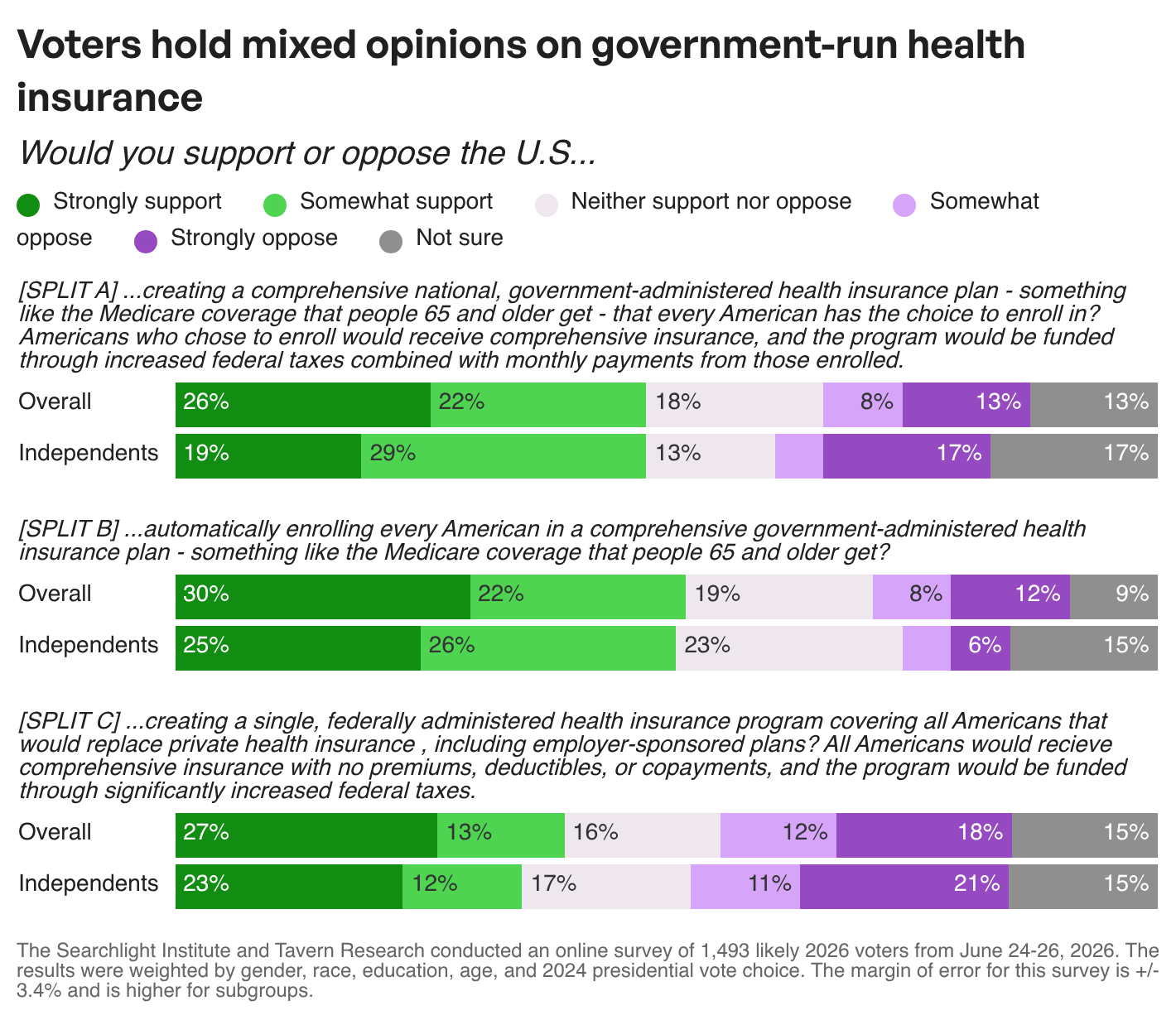
My biggest takeaway from these results is that Medicare for All is not a surefire political winner; it only cracks the majority of support in one of our questions, and support declines as you provide more information about the proposal. Many advocates will insist this can be fixed with messaging, but our research shows that policy design matters far more than any messaging.
Our first question asked voters about their support for a robust public option (a policy Searchlight supports): 48% of all voters say they would strongly or somewhat support such a proposal — while 18% say they would neither support nor oppose and 21% say they would somewhat or strongly oppose.
Our second question asked about automatically enrolling Americans in a comprehensive single-payer plan, but with soft language that didn’t specify replacing private insurance: 52% of all voters say they would strongly or somewhat support such a proposal — while 19% say they would neither support nor oppose and 20% say they would somewhat or strongly oppose.
Our third question asked if voters would support the government replacing all Americans’ private health insurance with a single federal health insurance program: 40% of all voters say they would strongly or somewhat support such a proposal — while 16% say they would neither support nor oppose and 30% say they would somewhat or strongly oppose.
Why did support fall off so much for the last policy proposal?
Voters trust their insurance and don’t trust the government
The single-biggest and perpetually undiscussed reason why we don’t have Medicare for All in this country is that the vast majority of Americans are satisfied with their health insurance plan. That doesn’t mean they don’t have issues with the health care system in general (most will say the system as a whole is broken), but that they are generally okay with the coverage they personally receive. Americans also trust their doctors and insurers more than they trust the federal government. The idea of switching off their current plan to one run by the government taps into both fear of uncertainty and loss aversion.
Candidates sometimes do this dance where they avoid saying they want to eliminate private insurance, either by describing niche cases where it would still be allowed (“supplementary” plans, or occasionally union insurance plans) or by describing Medicare for All as a public option that just naturally supplants private insurance. For example, Michigan Senate candidate Abdul El-Sayed evolved his Medicare for All position from outright abolishing private health insurance to automatically enrolling everyone under 65 in a comprehensive single-payer health plan. In his new model, private insurance would still exist, but it would be redundant compared to the comprehensive public plan that has no premiums, copays, or deductibles. This constant redefining of Medicare for All makes it frustrating to poll, since the policy details are contentious and ever-changing.
As you can see in our poll above, a fully described M4A plan is the least popular option we polled. As I said before, this has been my experience across years of polling this issue. Voters like the idea of reforms and government intervention, but are uncomfortable with tradeoffs like the loss of private insurance. They’re also likely confused about what Medicare for All means, since the term has been used for several different policies by different politicians.
Gut checking
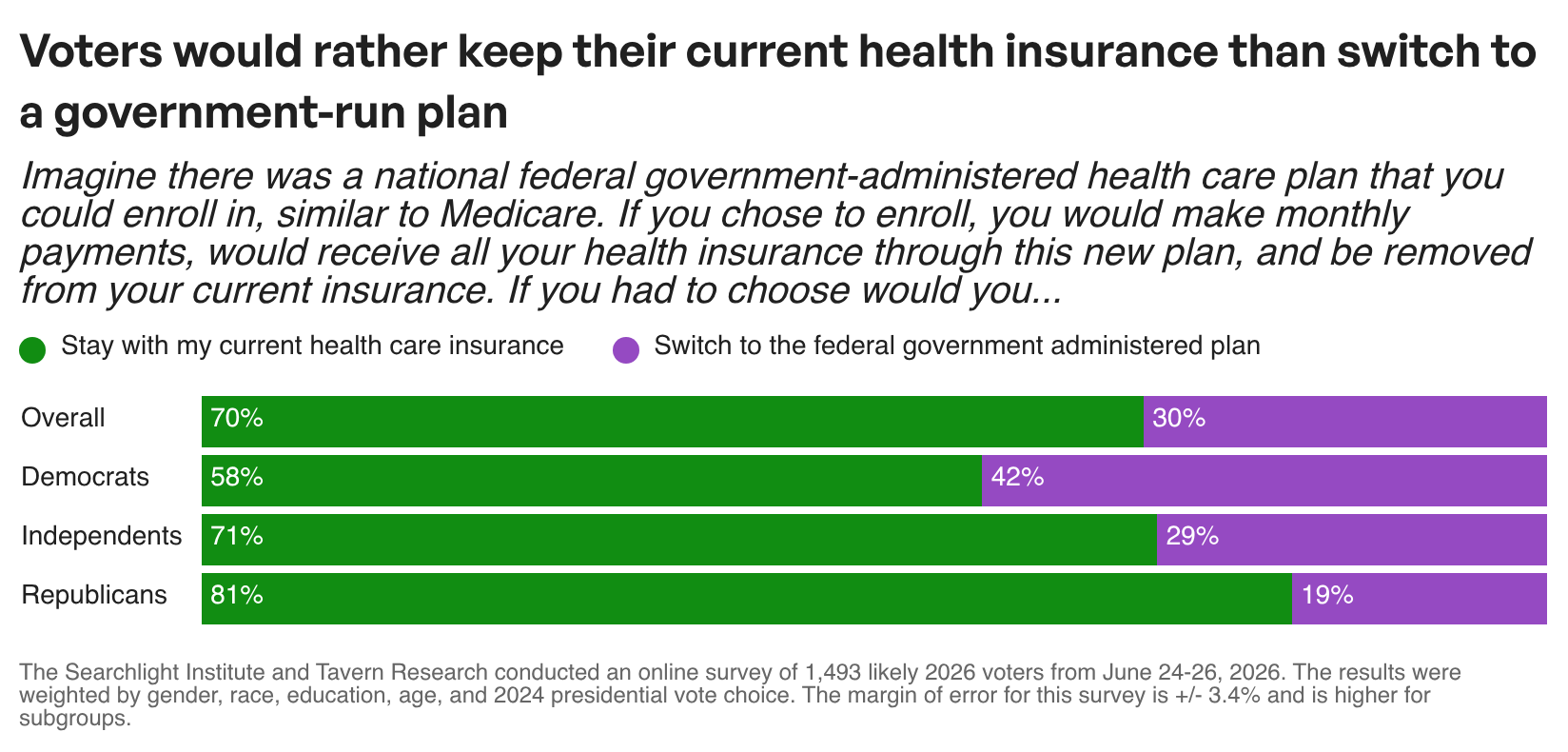
Asking about general support for government health care programs can be a bit abstract — after all, none of these are likely to become law any time soon. To get a more grounded read, we asked voters to imagine that there was a government-run health insurance program being offered to them today, and to decide if they would switch from their current insurance. The result was a resounding “no” from 70% of voters. This result was strong across majorities in all political affiliations, but was the most significant among Independents and Republicans.
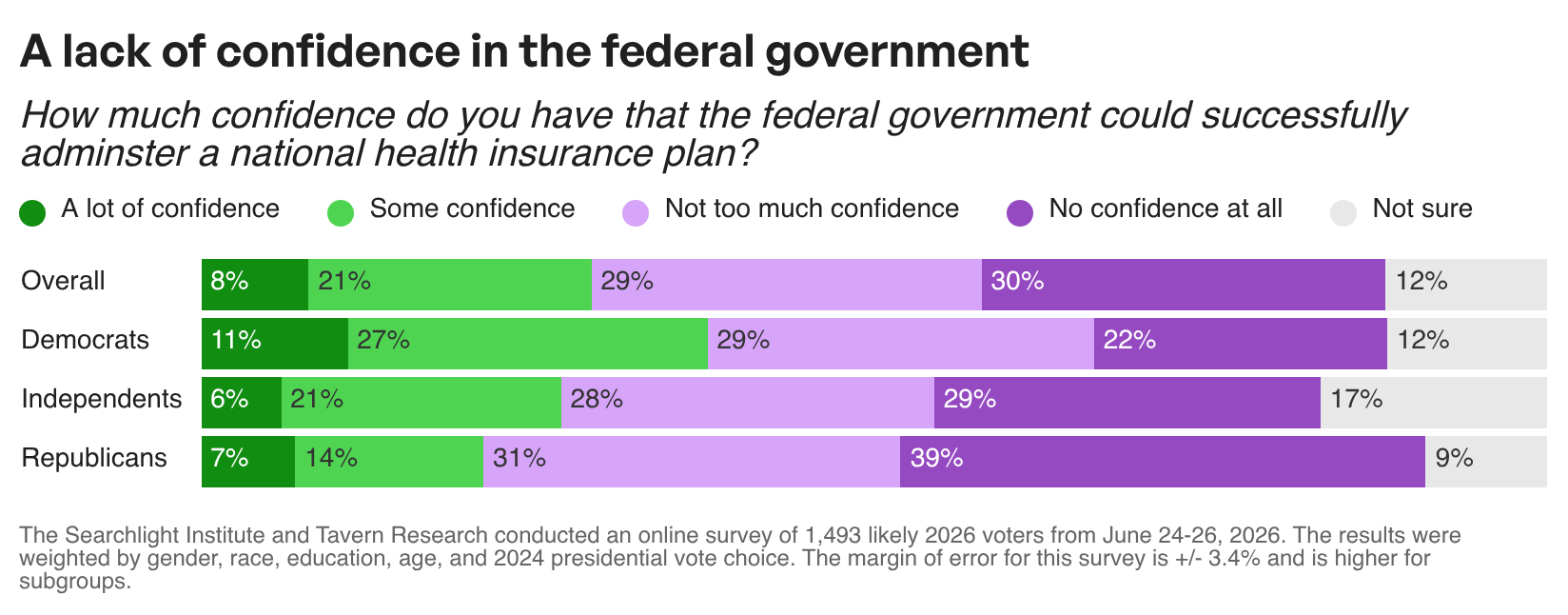
The explanation here is twofold. First, voters are overwhelmingly satisfied with their current insurance. Second, fifty-seven percent of voters do not trust the federal government to successfully administer a national health insurance plan. The number of voters, across parties, with “a lot of confidence” in the federal government is just paltry.
I’m not a health care policy wonk. David Bowen, our senior health care fellow, will be writing more about his plan to make coverage more affordable and more available over the following days. I have, however, spent a ton of time thinking about and measuring American public opinion. It would be a mistake to read Americans’ frustration with the health care system as an endorsement of a government takeover of that system when they’re even more frustrated with the government itself. Advocates for a greater governmental role in the system need to start by proving the government is competent. Until then, voters will keep choosing the option they know (private insurance) over a public option run by a government they don’t have confidence in. Advocates for Medicare for All face a second hurdle as well — overcoming voters’ discomfort with higher taxes and expensive new programs. Our polling makes it clear that voters want reforms to the health care system. The details are, as always, more complicated.
It seems like M4A/single-payer has displaced the public/government option (aka Medicare for Anyone, Medicare for All Who Want It) in terms of mindshare and chatter. Why is that?
There seems to be this fallacy on the Left that if you force the wealthy and privileged into the same systems as everyone else, they will use their wealth and privilege to improve that system. It seldom actually works that way; it seems naive to think that.
I would think that a public option that anyone could buy into at a reasonable price, taking into account personal resources (that is, means-tested premiums) and taking those who are actuarially uninsurable at reasonable rates, would solve a host of problems.
You wouldn't want the public option to become a "high risk pool" (although it wouldn't be the worst thing vs. the status quo if it did), and while you'd want the premiums to be competitive with private insurance where possible (one, to improve the risk pool with healthier people and two, keep Big Insurance on their toes and economically efficient), you wouldn't want to run private insurance out of business, to maintain that choice and also so private insurers can help to carry the load. There might need to be some regulation requiring private insurers to take on a certain number of higher risks to prevent dumping all of the high risks into the public option.
One other big benefit would be to combine Medicare, Medicaid, SCHIP, and everything else into one system (call it Americare) and reduce the overhead costs from separate administration.